Healthcare simulation faces the ongoing challenge of delivering high-quality education in an environment where medical knowledge and clinical protocols are continually evolving. Nowhere is this challenge more evident than in trauma care education, particularly in training for the recognition and management of tension pneumothorax. This HealthySimulation.com article by Dan Irizarry, MD, explores the pathophysiology of a tension pneumothorax and how effective clinical simulation with TacMed Solutions improves medical training.
Pathophysiology of Tension Pneumothorax
The pathophysiology of tension pneumothorax is well understood: air enters the pleural space due to blunt or penetrating trauma, or less commonly, spontaneous events such as a ruptured bleb. This air becomes trapped, leading to increased intrapleural pressure, collapse of the ipsilateral lung, and a shift of the mediastinum away from the affected side. The resulting impediment to venous return, with subsequent decline in cardiac output, can quickly become fatal without intervention.
Physiological compensation occurs early in the process, most notably through tachypnea, as the body attempts to overcome compromised gas exchange. Despite this, oxygen saturation (SpO₂) decreases as effective lung volume diminishes. Patients frequently present with anxiety, dyspnea, and visible respiratory distress initially.
TacMed will be a vendor at the 2025 ITSEC Optimizing Training: Ensuring Operational Dominance in Orlando, Florida, December 1 – 4, 2025. Visit them at Booth #1881.
As intrathoracic pressure continues to rise, hypoxemia worsens. End-tidal carbon dioxide (ETCO₂) also decreases, not due to ventilation failure, but as a consequence of reduced pulmonary perfusion and cardiac output, which limits CO₂ delivery to the alveoli. Declines in both SpO₂ and ETCO₂ are important indicators of progressive cardiorespiratory compromise.
Tachycardia is typically observed as the body attempts to sustain cardiac output in the face of worsening oxygenation and falling blood pressure. Without timely decompression, the patient’s mental status deteriorates, hypotension develops, and cardiac arrest becomes likely. Classic physical findings include decreased chest excursion and breath sounds on one side and, as a late sign, mediastinal shift.
| Stage | Heart Rate (HR) | Respiratory Rate (RR) | Oxygen Saturation (SpO2) | End-Tidal CO2 (ETCO2) | Other Clinical Signs | Blood Pressure (BP) |
|---|---|---|---|---|---|---|
| Early | Tachycardia (increased) | Tachypnea (increased) | May be near normal or slightly decreased | May be normal or slightly decreased | Chest retractions, Cyanosis, Jugular venous distension | May be normal or slightly increased |
| Progressing | Tachycardia (increased) | Severe increased rate, shallow breathing | Decreased (hypoxia) | Decreased due to poor ventilation | Severe shortness of breath | May begin to decrease as cardiac output drops |
| Late | Tachycardia progressing to bradycardia or weak pulse | Respiratory distress worsening | Significantly decreased | Significantly decreased | Hypotension, altered mental status, loss of consciousness | Significant hypotension due to obstructive shock |
View the HealthySimulation.com Webinar Mastering Airway and Respiratory Management Trauma Simulations and Visit the TacMed Solutions Vendor Directory Page to watch all their previous webinars!
Management of Open Chest Wound
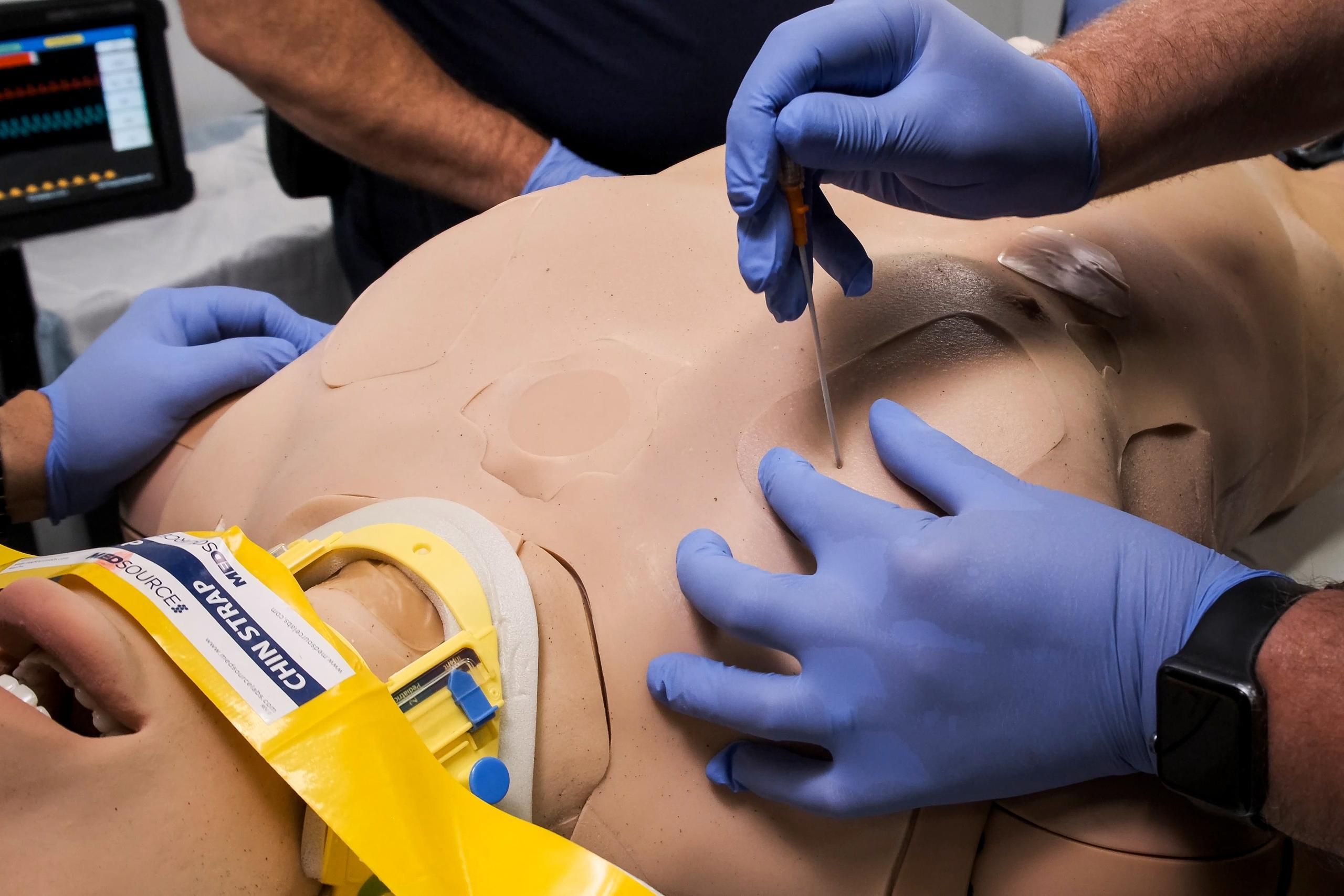
Immediate management begins with sealing open chest wounds before decompressing the pleural space. Needle thoracostomy is standard, though the specific technique varies by guideline. The European Trauma Course (ETC) recommends needle insertion at the second intercostal space, midclavicular line with a 14- or 16-gauge extra-long needle, while Advanced Trauma Life Support (ATLS) advises using a 5 or 8-cm needle at the fourth or fifth intercostal space, anterior midaxillary line. Diverging recommendations on technique, site, and equipment contribute to clinical uncertainty, especially when urgent action is required. Much of the evidence focuses on short-term outcomes, so longer-term safety, procedural risks, and the need for repeat interventions remain less characterized. A comprehensive synthesis of the available literature is essential to clarify best practices and guide future research.
View the new HealthySimulation.com Community Trauma Simulation Group to discuss this topic with your Global Healthcare Simulation peers!
Effective Clinical Simulation for Tension Pneumothorax Management
Structured approaches such as S.O.R.T. (Scenario, Objectives, Resources, Timing) canoptimize simulation-based training. In the context of tension pneumothorax, simulations shouldfoster skills in identifying at-risk patients, recognizing clinical deterioration through respiratoryand hemodynamic signs (including changes in respiratory rate, SpO2, and ETCO2), performingnecessary interventions, and evaluating responses to treatment.
Effective simulation requires realistic scenarios, appropriate task trainers, and opportunities forlearners to assess and manage evolving clinical presentations. Simulated patients should allowtrainees to practice anatomical landmarking on both anterior and lateral chest walls, as well asthe technical steps of needle or finger thoracostomy. The progression of simulated cases shouldreflect the typical evolution of tension pneumothorax over time, including early and late presentations.
Clinical Simulation Curricula
Simulation curricula should strive to align with current evidence and best practice guidelines, yet also prepare learners to adapt to local protocols and resource limitations, as institutional and regional differences are common. Simulation remains a critical modality for developing procedural competence in tension pneumothorax management. The realism and durability of task trainers directly influence educational outcomes. For instance, trainers such as the TacMed Clinical Response Upper can facilitate instruction and practice by providing key features, such as accurate anatomical landmarks for multiple decompression sites, tissue realism for procedural feedback, and the capacity for repeated use with consistent responses. Such resources help bridge the gap between theoretical knowledge and applied clinical skill, supporting the overarching goal of simulation-based education: safe, effective patient care.
More About TacMed Solutions
TacMed Simulation, an integral part of TacMed Solutions (aka TacMed), provides state-of-the-art training solutions with high-fidelity manikins to support improving survivability in response to crisis situations in the prehospital realm. Designed to offer first responders and military medics the most realistic medical training experience, the life-like simulators provide users with an autonomous response to field treatment, creating an immersive training environment. The training experience provides the confidence and expertise to effectively work under stressful conditions.
Each TacMed Simulation product is handcrafted in the USA and is designed from the ground up for ruggedness and durability with careful consideration of materials and manufacturing processes to create products that last. Learn more about the complete TacMed Solutions portfolio at tacmedsolutions.com.